Abstract
The goal. The goal of the work was to study the structure of viral and non-viral infections in patients with ischemic stroke, as well as the relationship between neurological recovery and severity of cerebral atherosclerosis, depending on the type of infectious agent.
Materials and methods. A total of 89 patients with ischemic acute cerebral circulation disorder and a history of clinical manifestations of a viral infection in the 3 months prior to the cerebrovascular accident were included in the study. Among the patients 44 (44.9%) were men and 54 (55.1%) were women with an average age of 62.08 ± 1.29 years (from 36 years to 92 years). 61 (81.9%) patients were diagnosed with ischemic stroke, and 28 (18.1%) patients were diagnosed with TIA.
The diagnosis was confirmed by magnetic resonance imaging (MRI), and the severity of neurological status was assessed using the National Institute of Health Stroke Scale (NIHSS) on the first, 7th and 21st day. Patients' blood serum was examined for the presence of herpes viruses DNA, the RNA of influenza viruses, enteroviruses, the viruses of an acute respiratory infection (adenoviruses), as well as for the common non-viral infections: mycoplasma, ureoplasma, toxoplasma, and chlamydia. The method of polycytomerase chain reaction (PCR) for DNA and RNA viruses extraction from blood serum (6; 8) and the method of enterovirus antigens detection in a cell culture by enzyme-linked immunosorbent assay (ELISA) (21; 24; 40) were used.
The degree of cerebral atherosclerosis was determined by ultrasound duplex scanning (UDS) of brachiocephalic arteries.
Methods of descriptive statistics were used.
Research results. The average period from the clinical manifestation of the infection to the development of stroke in patients with viral persistence was 11.8 ± 2.5 days (from 1 day to 90 days). Up to 7 days — 32 (36.0%) patients, from 7 days to 14 days inclusive — 44 (49.4%), more than 14 days — 13 (14.6%).
There was a weak but definite inverse correlation between the term of the viral manifestation and the severity of the acute cerebrovascular accident (r = 0.237, p = 0.025).
HSV1 (51) was detected most often in the acute period of stroke in 57% of patients, (p <0.05). The persistence of HSV2 and HHV6 was 38.2% and 32.6% respectively. A combination of two different HSV2 and HHV6 viruses was observed in 84 (89.9%) patients.
The combination of HSV1 / HSV2 is most commonly observed (in 29 (32.6%) patients p <0.05).
Coefficients of correlation between the presence of certain types of viruses, the number of stenoses, and the number of hemodynamically significant stenoses ranged from 0.19 with ARI to 0.33 in the case of a combination with HHV6.
There was no detectable relationship between the severity of neurological deficiency on the first day after the stroke and the type of viral infection or a combination thereof, except for adV (r = 0.27, p = 0.01).
The reduction in the NIHSS score on the 7th and the 21st day negatively correlated with the presence of certain viruses and their combinations, in particular herpesviruses or their associations HSV1, HSV1,2; HSV1,2-HHV6.
Conclusion. The DNA of HSV1, HSV2, HHV6, HHV4, HHV5 viruses was most often found in patients with ischemic stroke and a clinical manifestation of a persistent viral infection in history (within 1-90 days before the development of symptoms),
The presence of major vessels stenosis in the extracranial unit, the number of stenoses, and the presence of hemodynamically significant stenoses correlated with the presence of viral persistence of HHV6 and / or the association of HHV6 and influenza.
The presence of HSV1, HSV2, HHV6 viruses and / or their associations worsens the restoration of neurological functions in the acute post-ischemic period setting.
Introduction
The causes of atherosclerotic plaque (AP) destabilization, which lead to acute cerebral clinical manifestations of atherosclerosis (AS), such as ischemic stroke (IS), are not entirely known and are actively discussed by scientists [1].
There was a paradigm shift, as a result of which the theory that AS is a consequence of impaired cholesterol metabolism ceased to exist and a new one was established — regarding the inflammatory nature of the disease [2]. The source of such inflammation may be an infection [3]. The prediction of the association of infections and AS has a rational basis, because it is known that the process of development of atherosclerotic changes in the vascular wall includes chronic slow-progressing inflammation [4]. The ability of chronic infections to cause inflammation in tissues may be the cause of the progression of AP [5, 6, 7].
To date, the literature describes and systematizes almost 250 risk factors for AS [8]. The analysis showed that all of them are, in one way or another, linked to a persistent viral infection, which then links them to AS [9].
Based on the fact that AS is a multifactorial disease, the most likely risk factor (RF) is the “viral load” [10]. According to the "infectious overlay" hypothesis, atherosclerotic changes may occur under the conditions of a simultaneous persistence of several infections in patients with a lowered immunoreactivity, a pre-existing genetic predisposition, and other RFs; particularly, a combination of infections is more likely to be associated with stroke risk [11].
To date, the link between infections and AS can be considered proven, although much remains unclear in the pathogenesis [12]. In particular, this applies to the time interval between the signs of clinical manifestations of viral infection and the development of stroke.
Many studies have focused on the time period between the manifestations of viral infection and the onset of stroke; the estimated time between the viral infection and the emergence of stroke differs from author to author (Nagel M.A., Sreenivasan N., 2008, 2013). Most commonly the neurological symptoms of stroke occurred within one day to 1 month after varicella zoster virus (VZV) or herpes zoster (HZ) [13, 14]. According to Nagel M.A., Sreenivasan N. (2011, 2013) [14, 15, 16] an increased risk of stroke after HZ is most often observed after 3 months. A longer period was observed only in people who underwent HZ at a young age [14]. An analysis of 30 cases of an acute cerebrovascular accident (ACVA) associated with HZ showed the onset of neurological symptoms of stroke within 2.5 months after the appearance of a rash [15, 17]. The risk of stroke was considered the highest after 4 weeks (1.63), after 5-12 weeks (1.42), after 13-26 weeks (1.23). It is noted that in 55% of people receiving antiviral therapy for HZ the risk of a stroke incidence was reduced compared with untreated patients [18].
The connection between an infection and an occurrence of stroke can be observed throughout the different stages of cerebrovascular disease. The effect of infection and inflammation on the subtype of stroke, the lesions of large cerebral arteries, and the development of cardiogenic embolism (especially in patients without vascular RF) [19, 20] is stated; it is also noted that atherothrombotic and cardioembolic strokes frequently occur in patients who have suffered from respiratory infections [11, 21, 22, 23, 24].
To date, the association of infections and AS can be considered a proven fact, although the mechanism of pathogenesis remains unclear. The development of the "infectious" direction in the study of the IS gained momentum due to the accumulation of data on AS as a chronic inflammatory process initiated by vascular damage caused by various factors: from hypertension and smoking, to hyperhomocysteinemia and infectious pathogens [7, 25, 26, 27]. A common hypothesis connects chronic endothelial damage to bacterial and viral infections, free radicals activity, lowered nitric oxide levels, etc. Most likely, these factors that lead to the atherosclerotic process are interrelated and are links of the same chain [28].
The causes of destabilization of AP that lead to the occurrence of such clinical manifestations of AS as IS are actively discussed; clinical cases of coronary and cerebral atherothrombosis have been described, along with arterial and venous thrombosis localized elsewhere and associated with active herpesvirus infection, such as in patients with lowered and normal immunity [29, 30, 31]. At the same time, questions about the role of certain types of a viral infection in the implementation and the acceleration of the atherosclerotic process are insufficiently covered in the literature [2, 32, 33]. Virtually nothing is known about the effect of HHV types 3,6,7 and 8 on the pathogenesis of AS [33]. On the contrary, according to Y.Shi, O.Tokunaga, cytomegalovirus is more common in areas affected by AS compared to control areas: 40 vs. 4%, respectively. Also in the study of 33 samples of aortic tissue by PCR (10 of them with histological indications of AS), HSV type 1 was significantly more common in the group with histological indications of AS compared with samples of aorta without such indications (80 vs. 13%, respectively) [17]. In other cases no correlation was found between the presence of cytomegalovirus DNA (CMV) DNA and the structure of atherosclerotic plaques in carotid arteries. CMV was detected only in half of the artery samples [34]. The association between stroke and adenoviral infection has been described relatively recently [35]. The data from Kutleza M. et al. (2009), [35] indicate the association of stenotic arterial lesions with the presence of adenoviral infection. The risk of a primary stroke is significantly higher within the first 3 days after an acute infection and remains significantly elevated for 3 months [32].
So far the question of the proportion of different types of viral infection in patients with ischemic stroke developed after a manifested viral infection and the recovery of neurological deficit depending on the type of viral persistence has not been studied.
The goal of the study was to study the structure of viral and non-viral infections in patients with ischemic stroke, as well as the relationship between neurological recovery and severity of cerebral atherosclerosis, depending on the type of infectious agent.
Aim
Was to study the structure of viral and non-viral infections in patients with ischemic stroke, as well as the relationship between neurological recovery and severity of cerebral atherosclerosis, depending on the type of infectious agent.
Materials and methods
The study was conducted during 2015-2019 and set in Neurology departments of Oleksandrivska Hospital and Kyiv Medical Clinical Hospital № 4.
A total of 89 patients with acute ischemic stroke and anamnestic clinical manifestations of a viral infection within the 3 months before the vascular accident were included in the study. Among the patients 44 (44.9%) were men and 54 (55.1%) — women with an average age of 62.08 ± 1.29 years (from 36 years to 92 years old). An ischemic stroke was diagnosed in 61 (81.9%) of patients, and a transient ischemic attack (TIA) was diagnosed in 28 (18.1%) persons.
A stroke was confirmed by magnetic resonance imaging (MRI), and the National Institute of Health Stroke Scale (NIHSS) was used in diagnosis. The patients’ serum was examined for the presence of DNA of human herpes viruses: herpes simplex type 1 and 2 (HSV1, HSV2), Epstein-Barr (EBV), cytomegalovirus (CMV), HNV6, RNA of influenza virus (the flu), viruses of acute respiratory infection, adenoviruses, enteroviruses, as well as DNA of mycoplasma, ureaplasma, toxoplasma, and chlamydia.
The following virological research methods were used: the method of viral DNA and RNA detection in blood serum by polycytomerase chain reaction (PCR) [36, 37], and the method of detection of enteroviruses in a cell culture using an enzyme-linked immunosorbent assay (ELISA) [38, 39, 40].
All patients underwent ultrasound duplex scanning (UDS) of the brachiocephalic arteries on a Medison ACCUVIX V10 device with a phased 2-4 MHz sensor to determine the degree of stenosis, the thickness of the CIM in the internal carotid, common carotid, middle cerebral, anterior cerebral and posterior cerebral, vertebral (ICA, CCA, MCA, ACA, PCA, VA) and basilar arteries, respectively. The pathogenetic subtype of stroke was determined using TOAST criteria [41].
Results and discussion
The patients were divided by the pathogenetic subtype as follows: more than half of the patients — 50 (56.2%) were determined to have an atherothrombotic subtype (ATS), 9 (10.1%) patients had an cardioembolic (CE) subtype, 7 (7, 9%) had a lacunar (LAC) subtype, 12 (13.5%) patients had a hemodynamic (HD) subtype; a subtype was not definitively determined (NDD) in 11 (12.4%) patients.
Among the 89 patients with IS and TIA, 67 (64%) patients had lesions of the carotid arteries, including 32 (36.0%) patients with lesions in the left CMA and 22 (24.7%) patients with lesions in the right CMA.
It should be noted that the frequency of lesions of different vascular sources differed significantly in patients with stroke and with TIA. In the case of IS the lesions of carotid vessels were more common, specifically of the left and the right middle cerebral arteries (LCMA and RCMA); in the case of TIA – the lesions of the vertebrobasilar system (VBS) were more common, p = 0.042, Table 1.
| Affected artery | Stroke | TIA | Total | |||
|---|---|---|---|---|---|---|
| Abs. | % | Abs. | % | Abs. | % | |
| LCMA | 23 | 37.7 | 9 | 32.1 | 32 | 36.0 |
| RCMA | 19 | 31.1 | 3 | 10.7 | 22 | 24.7 |
| VBS | 16 | 26.2 | 16 | 57.1 | 32 | 36.0 |
| RICA | 1 | 1.6 | 0 | 0 | 1 | 1.1 |
| R+L CMA | 2 | 3.3 | 0 | 0 | 2 | 2.2 |
| Total | 61 | 100.0 | 28 | 100.0 | 89 | 100.0 |
The severity of the neurological deficit according to NIHSS ranged from 7 to 15 points with an average of - 9.42 ± 0.26 points.
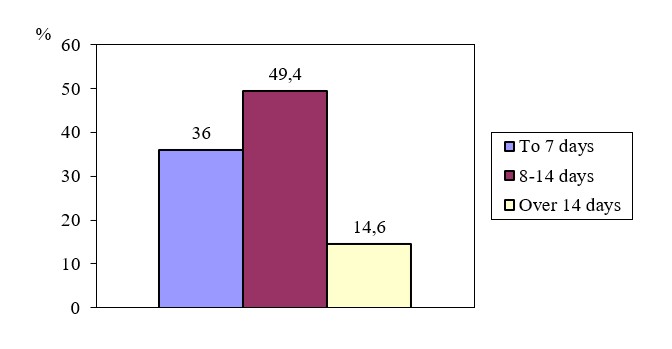
The mean time of clinical manifestation in patients with viral persistence was 11.8 ± 1.5 days (from 1 day to 90 days).
32 (36.0%) patients – in under 7 days; 44 (49.4%) patients – from 7 days to 14 days inclusively; 13 (14.6%) patients – more than 14 days.
Figure 1. The distribution of patients by the term of viral manifestation in the anamnesis before the occurrence of the vascular event
There was a weak but significant correlation between the time of viral manifestation and the severity of acute cerebral circulation disorder - r = - 0.237, p = 0.025.
Analysis of the distribution of patients depending on the type of viral persistence and their combinations shows that HSV1 (51) was most often detected in 57% of patients; more than a third of patients – 38.2% and 32.6%, respectively – had signs of HSV2 and HHV6 persistence. CMV-23.6% and EBV-28.1% were detected slightly less frequently. Almost one-fifth were patients infected with the flu (19.1%). Ureoplasma and mycoplasma was detected in approximately 15.7% and 16.9%, respectively, of the patients with a symptomatic viral persistence; and chlamydia and toxoplasma — in 9% and 10.1% of cases, respectively, Table 2.
| Virus | Abs. | % |
|---|---|---|
| HSV 1 | 51 | 57.3 |
| HSV 2 | 34 | 38.2 |
| HHV6 | 29 | 32.6 |
| EBV | 25 | 28.1 |
| CMV | 21 | 23.6 |
| Flu | 17 | 19.1 |
| Mycoplasma | 15 | 16.9 |
| Ureoplasma | 14 | 15.7 |
| Toxoplasma | 9 | 10.1 |
| Chlamydia | 8 | 9.0 |
| Adenovirus | 3 | 3.4 |
| Enterovirus | 2 | 2.2 |
| Acute respiratory viral infection | 1 | 1.1 |
It should be noted that there was a combination of two different viruses in 84 (89.9%) patients, and three viruses (HSV 1 + HSV 2 + HHV6) – in 6 (6.7%) patients. In patients that had a combination of two viruses, the following were observed: HSV1 — in 38 (45.2%) patients, the flu — in 34 (40.5%) patients, and HHV6 — in 34 (40.5%) patients. The most common combination of HSV1 + HSV2 was observed in 29 (32.6%) patients, all p <0.05, Table 3.
| Combinations | Abs. | % |
|---|---|---|
| HSV1/HSV2 | 29 | 32.6 |
| HHV6/Flu | 13 | 14.6 |
| HHV6 +EBV | 11 | 12.4 |
| HHV6+ CMV | 10 | 11.2 |
| HSV1+Flu | 9 | 10.1 |
| EBV+Flu | 7 | 7.9 |
| HSV2+Flu | 5 | 5.6 |
62 patients (63.4%) hospitalized with signs of viral persistence in the anamnesis were diagnosed with stenotic lesions of cerebral vessels. Moreover, in more than half of the cases, or 38 (57.9%) patients, lesions of two vascular areas were determined. In 12 patients (21.1%) a lesion of one vascular area was detected; in 11 (19.3%) patients three areas were affected; and four areas — in 1 (1.8%) patient.
Among the vessels affected by atherosclerotic stenosis, the largest percentage belonged to the main vessels of the head and neck in the extracranial part. Stenosis of RCCA and LCCA was 22.1 and 21.3% of RICA and LICA, respectively, — 19.7%; meaning, more than 80% of vessels with stenosis were common and internal carotid arteries.
In patients with vascular stenosis more than half (63.2%) were patients with a detected hemodynamically marked stenosis in an at least one vessel.
It was found that the presence of stenosis significantly correlated with certain types of viruses or with their associations, Fig. 2-4.
Figure 2. Correlation coefficients between the presence of a viral persistence and the presence of extracranial vessel stenosis
The correlation coefficients between the presence of certain types of viruses and the number of stenoses ranged from 0.19 in ARVI to 0.25, as in the case of a combination of HHV6 + flu.
Correlations between certain types of viruses and the number of hemodynamically marked stenoses were also revealed, Fig. 3.
Рисунок 3. Correlation coefficients between the presence of viral persistence and the number of hemodynamically marked vascular stenoses
| Virus | r | p |
|---|---|---|
| HSV1 | 0.035 | 0.748 |
| HSV2 | 0.011 | 0.922 |
| HHV6 | 0.144 | 0.179 |
| CMV | 0.035 | 0.747 |
| EBV | 0.026 | 0.808 |
| Enterovirus | 0.056 | 0.604 |
| Ureaplasma | 0.064 | 0.551 |
| ARVI | 0.103 | 0.336 |
| Mycoplasma | 0.075 | 0.485 |
| Chlamydia | 0.105 | 0.327 |
| Toxoplasma | 0.079 | 0.464 |
| Adenovirus | 0.268 | 0.011 |
| Flu | 0.137 | 0.201 |
| HSV1+ HSV2 | 0.001 | 0.996 |
| HSV1+HSV2+ HHV6 | 0.117 | 0.275 |
| HHV6+Flu | 0.148 | 0.167 |
| HHV6+EBV | 0.156 | 0.143 |
| HHV6+CMV | 0.026 | 0.807 |
| ЕВV+Flu | 0.085 | 0.427 |
| HSV1+Flu | 0.041 | 0.703 |
| HSV2+Flu | 0.041 | 0.705 |
| HSV1+ HSV2 | 0.001 | 0.996 |
The dynamics of the neurological deficit was positive in 86.4% of patients. An average decrease of the NIHSS scores on the 7th day was 17.9 ± 1.1% (maximum 36.4%), and ranged from 6 to 14 points, with an average of 8, 8 ± 0.22 points.
A percentage reduction of the NIHSS scores on 7th day was to some extent inversely correlated with the presence of a viral infection; this means that the persistence of certain types of viruses or their associations inhibited the restoration of neurological functions, Figure 4.
Figure 4. The absolute value of a statistically significant (p <0.05) correlation coefficient between the presence of viral persistence and the percentage decrease of the NIHSS scores on the 7th day
The most negative effect on the restoration of neurological functions at the end of the acute period of stroke resulted from the presence of herpesviruses: HSV1, association HSV1 + 2 or HSV1 + HSV2 + HHV6.
A negative correlation between the percentage reduction in the score of neurological deficit with the presence of a certain type of virus was observed at the end of the acute period at the 21st day, although with lower correlation coefficients, Figure 5.
Рисунок 5. The absolute value of the correlation coefficient (in the case of its statistically significant value, p <0.05) between the presence of a viral persistence and the percentage decrease of NIHSS scores on the 21st day
Thus, the study of the proportion of different types of viruses (both herpes and the flu), acute respiratory infection (adenoviruses), enteroviruses, and some common infections of non-viral origin in patients with IS with signs of acute infection in the anamnesis within 3 months prior to an emergence of a vascular disorder showed that more than half of patients (51) 57% had HSV1, and more than a third of patients (38.2% and 32.6%) suffered from HSV2 and HHV6, respectively. It should be noted that more than 50% of patients with signs of viral manifestations in the anamnesis showed a combination of two different viruses, and significantly more often a combination of HSV1 + HSV2 was observed.
Changes in the properties of AP under the influence of acute infection may lead to a degradation of its stability, resulting in thrombosis, embolism, and a development of clinical manifestations of TIA /IS, which remain the subject of an active discussion [42].
In regard to this, an important goal of this study was to research the frequency of stenotic lesions of cerebral vessels, as well as their severity. More than half of the patients with stroke and a demonstrated viral persistence (64.0%) were diagnosed with stenosis of cerebral and precerebral vessels, and 58% of patients had two vascular areas affected by the atherosclerotic process. Among the patients diagnosed with stenotic vascular lesions, 48 (63.2%) patients had hemodynamically marked stenosis of an at least one vessel, which is more than half (53.9%) of the total number of patients. It was found that the number and the presence of a hemodynamically significant stenosis correlated with a detected viral infection. The obtained data is clearly evident not only of the connection between the viral infection and the atherosclerotic process activity in patients, but, likely, also demonstrates the uniqueness of the effect of a particular virus on the course of a cerebral atherosclerosis. There is a notion linking the severity and the negative consequences of IS to a prior infection, including a viral infection [43, 44, 45, 46, 47, 48]. According to the analysis of the obtained data, the percentage reduction in the score of neurological deficit according to NIHSS on the 7th day and on the 21st day (relative to the values on the first day) was inversely correlated with the presence of some viruses and their associations: HSV1,2; XXV6 + CMV; HHV6 + flu; that is, the presence of certain viruses or their associations exacerbated the regression of neurological deficits in the acute period of stroke.
Conclusions
Most often in patients with both an ischemic stroke and clinical manifestations of a persistent viral infection in the anamnesis (1–90 days prior to the development of symptoms) the DNA of HSV1, HSV2, HHV6, EBV, and CMV viruses were detected.
The presence of a main vessel stenosis in the extracranial region, the number of stenoses and the presence of hemodynamically significant stenoses correlated with the presence of HHV6 viral persistence and / or with the persistence of an association of HHV6 and flu.
The presence of HSV1, HSV2, HHV6 viruses and / or their associations impairs the restoration of neurological functions in the setting of an acute post-stroke period.
References
- Breuer J, Pacou M, Gautier A, Brown MM. Herpes zoster as a risk factor for stroke and TIA: a retrospective cohort study in the UK. Neurology. 2014;83(2):e27-e33. DOI: 10.1212/WNL.0000000000000038. PMID: 24384645.
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685-95. DOI: 10.1056/NEJMra043430.
- Hug A, Dalpke A, Wieczorek N, et al. Infarct volume is a major determiner of post-stroke immune cell function and susceptibility to infection. Stroke. 2009;40(10):3226-32. DOI: 10.1161/STROKEAHA.109.557967. PMID: 19661470.
- Gomez E, Laures A, Baltar JM, Melon S, Dı́ez B, De Ona M. Cytomegalovirus replication and “herpesvirus burden” as risk factor of cardiovascular events in the first year after renal transplantation. In Transplantation proceedings. 2005;37(9):3760-3.
- Abakumova YuV, Ardamatskiy NA. Morfologicheskie, funktsionalnyie, infeektsionnyie aspektyi aterogeneza. Mezhdunarodnyiy meditsinskiy zhurnalyu. 2000;(6):522-4.
- Vinichuk SM, Cherenko TM. Ishemicheskiy Insult: evolyutsiya vzglyadov na strategiyu lecheniya. Kyiv: Kosmopolis; 2003:120.
- Gafurov BG, Rakhmanova SP. Some clinical-pathological characteristics of the first and recurrent cerebral stroke. Mezhdunarodnyiy nevrologicheskiy zhurnal. 2011;(1):59-62.
- Manousakis G, Jensen MB, Chacon MR, Sattin JA, Levine RL. The interface between stroke and infectious disease: infectious diseases leading to stroke and infections complicating stroke. Curr Neurol Neurosci Rep. 2009;9(1):28-34. DOI: 10.1007/s11910-009-0005-x. PMID: 19080750.
- Hiryna OM. Imunopatohenetychni ta endokrynni zminy pry riznykh formakh ishemichnoi khvoroby sertsia v umovakh virusnoi infektsii i yikh terapevtychna korektsiia. Kyiv: Kosmopolis; 1996.
- O'Connor S, Taylor C, Campbell LA, Epstein S, Libby P. Potential infectious etiologies of atherosclerosis: a multifactorial perspective. Emerg Infect Dis. 2001;7(5):780-788. DOI: 10.3201/eid0705.010503. PMID: 11747688.
- Elkind MS, Ramakrishnan P, Moon YP, et al. Infectious burden and risk of stroke: the northern Manhattan study. Arch Neurol. 2010;67(1):33-38. DOI: archneurol.2009.271. PMID: 19901154.
- Yarullina DR, Ilinskaya NI. Silkin MKh. Salakhov RN. Khairullin. infectious nature of atherosclerosis: facts and hypotheses. Uchenyie zapiski Kazanskogo gosudarstvennogo universiteta. 2010;152(Kn 1):136-154.
- Nagel MA, Cohrs RJ, Mahalingam R, et al. The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features. Neurology. 2008;70(11):853-860. DOI: 10.1212/01.wnl.0000304747.38502.e8. PMID: 18332343.
- Sreenivasan N, Basit S, Wohlfahrt J, et al. The short- and long-term risk of stroke after herpes zoster - a nationwide population-based cohort study. PLoS One. 2013;8(7):e69156. DOI: 10.1371/journal.pone.0069156. PMID: 23874897.
- Nagel MA, Traktinskiy I, Azarkh Y, et al. Varicella zoster virus vasculopathy: analysis of virus-infected arteries. Neurology. 2011;77(4):364-370. DOI: 10.1212/WNL.0b013e3182267bfa. PMID: 21753174.
- Nagel MA, Choe A, Khmeleva N, et al. Search for varicella zoster virus and herpes simplex virus-1 in normal human cerebral arteries. J Neurovirol. 2013;19(2):181-185. DOI: 10.1007/s13365-013-0155-0. PMID: 23456953.
- Span AH, Van Dam-Mieras MC, Mullers W, Endert J, Muller AD, Bruggeman CA. The effect of virus infection on the adherence of leukocytes or platelets to endothelial cells. Eur J Clin Invest. 1991;21(3):331-338. DOI: 10.1111/j.1365-2362.1991.tb01378.x. PMID: 21753174.
- Nagel MA, Gilden D. The relationship between herpes zoster and stroke. Curr Neurol Neurosci Rep. 2015;15(4):16. DOI: 10.1007/s11910-015-0534-4. PMID: 25712420.
- Loseva MI, Masyicheva VI., Beltsova AI., Kosmachyova TA. Opyit primeneniya ridostina dlya lecheniya grippa i ORVI. В: Materialyi kruglogo stola Primenenie ridostina dlya lecheniya virusnyih i bakterialnyih infektsiy i perspektivyi ego ispolzovaniya pri zabolevaniyah infektsionnoy prirodyi. Berdsk;1998:64-67.
- Maltsev DV. Herpesvirusni neiroinfektsii liudyny. Kyiv: Nats. med. un-t im. O.O. Bohomoltsia, In-t imunolohii ta alerholohii; 2014. 366 s.
- Kuznetsova SM. Faktoryi riska i profilaktika insulta. Likuvannia ta diahnostyka. 1998;(3):22-25.
- Marychev IL. Herpesvirusy 1 ta 2 typu–poshyrenist ta diahnostyka. Laboratorna diahnostyka. 2008;(3):18-21.
- Hosseinipour MC, Smith NH, Simpson EP, Greenberg SB, Armstrong RM, White AC. Middle cerebral artery vasculitis and stroke after varicella in a young adult. South Med J. 1998;91(11):1070-1072. DOI: 10.1097/00007611-199811000-00018. PMID: 9824195.
- Puskas LG, Tiszlavicz L, Rázga Z, Torday LL, Krenacs T, Papp JG. Detection of nanobacteria-like particles in human atherosclerotic plaques. Acta Biologica Hungarica. 2005;56(3-4):233-245.
- Zhukova YV, Masycheva VI, Nikitin YuP. The effect of acute respiratory viral infection on the coronary heat disease. Byulleten SO RAMN. 2008;(4): 56-59.
- Knobler SL, O'Connor S, Lemon SM, et al., eds. The Infectious Etiology of Chronic Diseases: Defining the Relationship, Enhancing the Research, and Mitigating the Effects: Workshop Summary. Washington: National Academies Press; 2004. DOI: 10.17226/11026. PMID: 22379643.
- Stassen FR, Vainas T, Bruggeman CA. Infection and atherosclerosis. An alternative view on an outdated hypothesis. Pharmacol Rep. 2008;60(1):85-92.
- Bobrychev YV.,Andreeva ER.,Michailova LA, et al. Correlation between lipid deposition ,immune-inAamatory cell content and MNC class II expression in diffuse intimal thickening of the human aorta. Aterosclerosis. 2011;219(1):171-183.
- Finn AV, Nakano M, Narula J, Kolodgie FD, Virmani R. Concept of vulnerable/unstable plaque. Arterioscler Thromb Vasc Biol. 2010;30(7):1282-1292. DOI: 10.1161/ATVBAHA.108.179739. PMID: 20554950.
- Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003. DOI: 10.1093/eurheartj/eht296. PMID: 23996286.
- Yasuda C, Okada K, Ohnari N, Akamatsu N, Tsuji S. Cerebral infarction and intracranial aneurysm related to the reactivation of varicella zoster virus in a Japanese acquired immunodeficiency syndrome (AIDS) patient. Rinsho Shinkeigaku. 2013;53(9):701-705. DOI: 10.5692/clinicalneurol.53.701. PMID: 24097317.
- Auer J, Berent R, Weber T, Eber B. Influenza virus infection, infectious burden, and atherosclerosis. Stroke. 2002;33(6):1454-1455. DOI: 10.1161/01.str.0000018667.77849.95. PMID: 12052970.
- Flamand L, ed. Human Herpesviruses HHV6A, HHV-6B & HHV-7: diagnosis and clinical management. 3rd ed. Oxford, UK: Elsevier; 2014. 368 p.
- Virok D, Kis Z, Kari L, et al. Chlamydophila pneumoniae and human cytomegalovirus in atherosclerotic carotid plaques-combined presence and possible interactions. Acta Microbiol Immunol Hung. 2006;53(1):35-50. DOI: 10.1556/AMicr.53.2006.1.3. PMID: 16696549.
- Kutlesa M, Tesović G, Knezović I, Mise B, Visković K, Barisić N. Ischemic stroke associated with adenoviral infection in a 4-year-old boy. Wien Klin Wochenschr. 2009;121(23-24):776-779. DOI: 10.1007/s00508-009-1286-4. PMID: 20047116.
- Huralia AL, Spivak OM. Praktychnyi posibnyk z imunofermentnoho analizu. Kyiv: Polimed; 2003. 51 s.
- Leneva IA, Fadeeva NI, Fedyakina IT. Primenenie immunofermentnoy indikatsii virusspetsificheskih antigenov v izuchenii novogo protivogrippoznogo preparata arbidola. Himiko-farmarmakologicheskiy zhurnal. 1994;(9):4-8.
- Graham FL, Van der Eb AJ. A new technique for the assay of infectivity of human adenovirus 5 DNA. Virology. 1973;52(2):456-467. DOI: 10.1016/0042-6822(73)90341-3. PMID: 4705382.
- Crowther JR The ELISA Guidebook. 2nd ed. Humana Press. 2009:566.
- Burke S, ed. PCR:DIOS Essential techniques. New York: John Wiley & Sons; 1996:153.
- Chapman N, Huxley R, Anderson C, et al. Effects of a perindopril-based blood pressure-lowering regimen on the risk of recurrent stroke according to stroke subtype and medical history: the PROGRESS Trial. Stroke. 2004;35(1):116-121. DOI: 10.1161/01.STR.0000106480.76217.6F. PMID: 14671247.
- Niessner A, Sato K, Chaikof EL, Colmegna I, Goronzy JJ, Weyand CM. Pathogen-sensing plasmacytoid dendritic cells stimulate cytotoxic T-cell function in the atherosclerotic plaque through interferon-alpha. Circulation. 2006;114(23):2482-2489. DOI: 10.1161/CIRCULATIONAHA.106.642801. PMID: 17116765.
- Grau AJ, Becher H, Ziegler CM, et al. Periodontal disease as a risk factor for ischemic stroke. Stroke. 2004;35(2):496-501. DOI: 10.1161/01.STR.0000110789.20526.9D. PMID: 14707235.
- Emsley HC, Hopkins SJ. Acute ischaemic stroke and infection: recent and emerging concepts. Lancet Neurol. 2008;7(4):341-353. DOI: 10.1016/S1474-4422(08)70061-9. PMID: 18339349.
- Hennerici MG. The unstable plaque. Cerebrovasc Dis. 2004;17 Suppl 3:17-22. DOI: 10.1159/000075300. PMID: 14730254.
- Macko RF, Ameriso SF, Gruber A, et al. Impairments of the protein C system and fibrinolysis in infection-associated stroke. Stroke. 1996;27(11):2005-2011. DOI: 10.1161/01.str.27.11.2005.PMID: 8898806.
- Paganini-Hill A, Lozano E, Fischberg G, et al. Infection and risk of ischemic stroke: differences among stroke subtypes. Stroke. 2003;34(2):452-457. DOI: 10.1161/01.str.0000053451.28410.98.PMID: 12574559.
- Palasik W, Fiszer U, Lechowicz W, Czartoryska B, Krzesiewicz M, Lugowska A. Assessment of relations between clinical outcome of ischemic stroke and activity of inflammatory processes in the acute phase based on examination of selected parameters. Eur Neurol. 2005;53(4):188-193. DOI: 10.1159/000086355. PMID: 15956787.